Sensitivity, Specificity, Positive and Negative Predictive Values | MarinStatsLectures
TLDRThe video by Mike Marin delves into the concepts of screening and diagnostic tests, emphasizing the importance of sensitivity, specificity, positive predictive value, and negative predictive value. It explains the differences between these tests, their purposes, and how they are used in healthcare. The video also demonstrates how to calculate these values using a 2x2 table and discusses the limitations of such calculations in certain study designs. The content is informative, aiming to enhance understanding of these critical healthcare assessment tools.
Takeaways
- 🔍 **Screening vs. Diagnostic Tests**: Screening tests are used for early identification of at-risk individuals without symptoms, while diagnostic tests confirm the presence or absence of a disease in symptomatic individuals or those with positive screening results.
- 💰 **Cost and Invasiveness**: Screening tests are typically cheaper and non-invasive, whereas diagnostic tests tend to be more expensive and invasive.
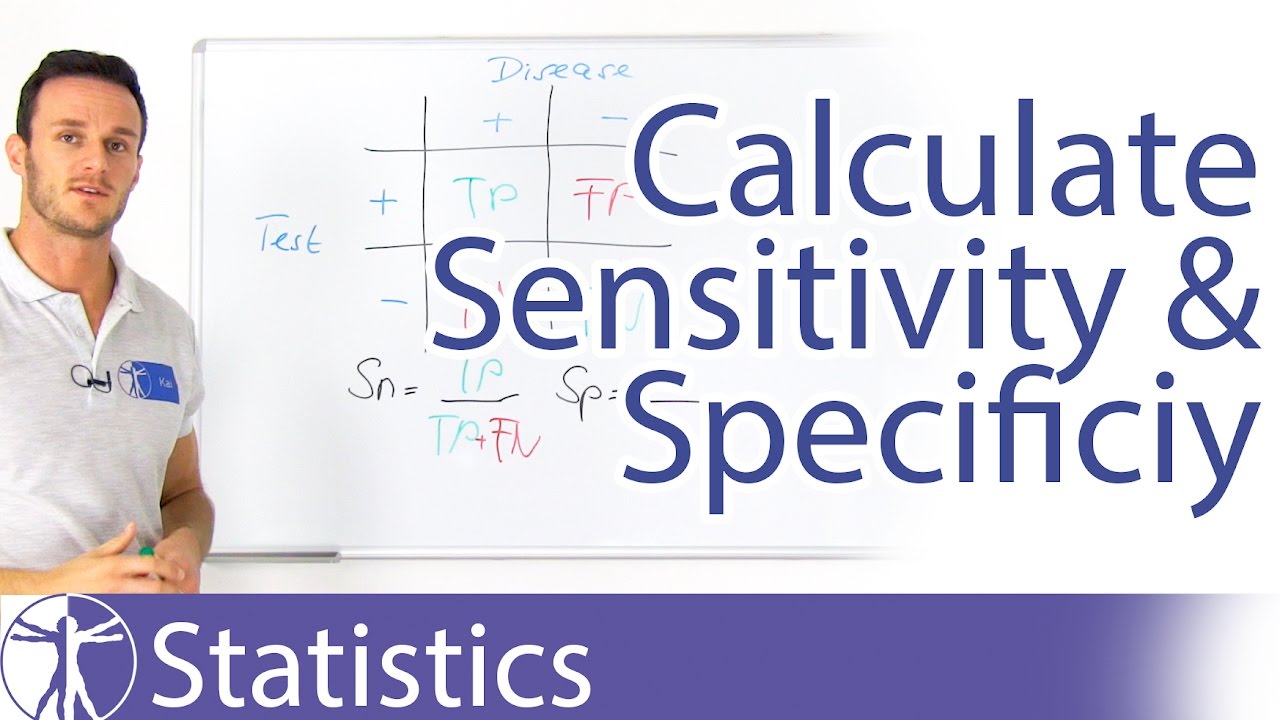
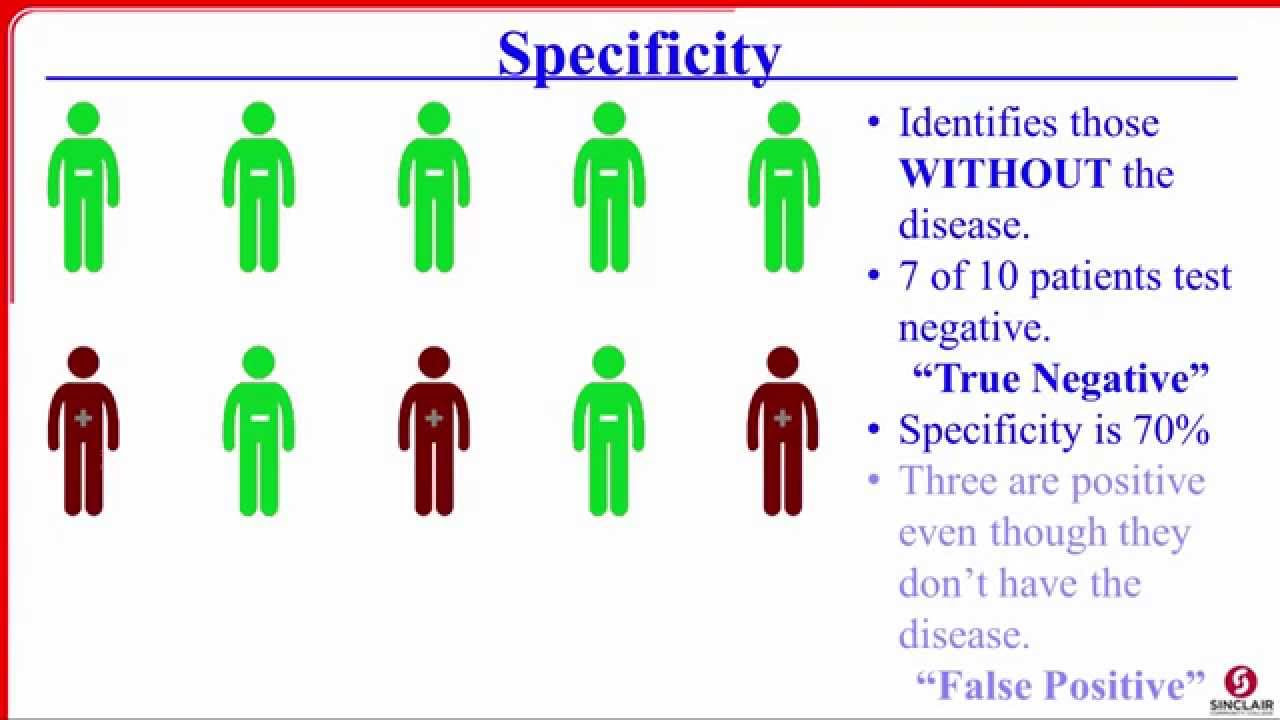
- 📈 **Sensitivity and Specificity**: Sensitivity is the likelihood of a true positive (correctly identifying a diseased individual), and specificity is the likelihood of a true negative (correctly identifying a non-diseased individual).
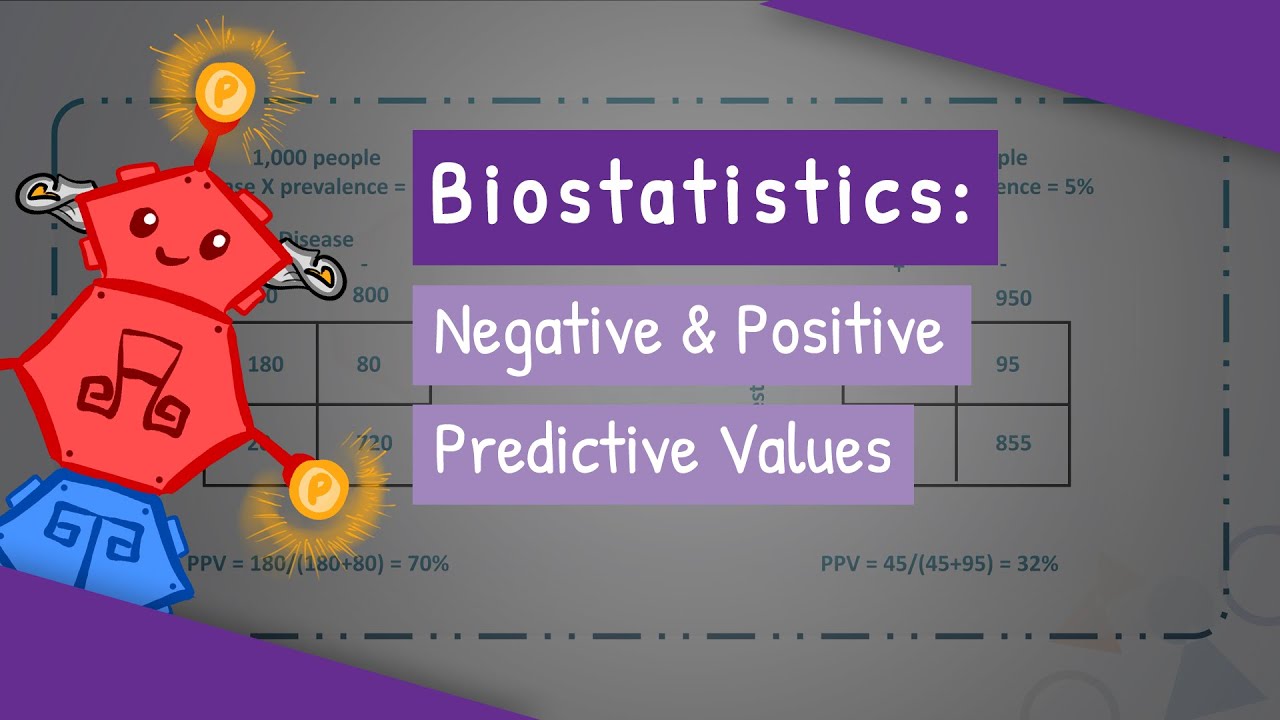
- 🔄 **Positive and Negative Predictive Values**: Positive Predictive Value (PPV) indicates the probability of actually having the disease given a positive test result, while Negative Predictive Value (NPV) indicates the probability of not having the disease given a negative test result.
- 📊 **2x2 Tables for Calculation**: Sensitivity, specificity, PPV, and NPV can be calculated using 2x2 tables, which require data on true positives, false positives, true negatives, and false negatives.
- 🔄 **Prevalence**: Prevalence is the proportion of individuals in a population with the disease and is used to estimate the likelihood of a positive or negative test result.
- 🌟 **Prospective vs. Case-Control Studies**: Prospective studies follow individuals over time to observe disease development, while case-control studies compare confirmed cases with non-cases, which may not represent the population prevalence.
- ⚖️ **Threshold Adjustment**: Adjusting the threshold for a positive test result can increase sensitivity (more true positives) but also increase false positives, thus affecting specificity.
- ⚠️ **Limitations of 2x2 Tables**: Using 2x2 tables to calculate PPV and NPV can be biased if the data is not collected prospectively or if the sample prevalence does not match the population prevalence.
- 🧠 **Understanding Test Reliability**: PPV and NPV help assess the reliability of test results, indicating how often a test correctly identifies the presence or absence of a disease.
- 📚 **Educational Value**: The video aims to educate viewers on the importance and application of sensitivity, specificity, PPV, and NPV in medical testing and decision-making.
Q & A
What is the primary purpose of screening tests?
-The primary purpose of screening tests is to identify individuals who may have a disease early on, before they start to show symptoms, particularly those who are considered to be at risk.
How do screening tests differ from diagnostic tests?
-Screening tests are used to screen individuals without symptoms but at risk of having a disease, aiming to identify them early. Diagnostic tests, on the other hand, are administered to confirm the presence or absence of a disease in individuals who are showing symptoms or have tested positive in a screening test.
What are the typical characteristics of screening tests in terms of sensitivity and cost?
-Screening tests tend to have higher sensitivity and higher false positive rates to not miss potential cases. They are also usually cheaper and non-invasive.
How is sensitivity defined in the context of medical testing?
-Sensitivity is defined as the probability of getting a positive test result given that the individual actually has the disease, essentially the likelihood of a diseased individual getting a correct positive diagnosis.
What is the complement of sensitivity called, and what does it represent?
-The complement of sensitivity is called a false negative, which represents the probability of an individual with the disease testing negative, failing to correctly diagnose a diseased individual.
How is specificity related to correctly identifying non-diseased individuals?
-Specificity is the probability of getting a negative test result given that the individual does not have the disease, indicating how often the test correctly identifies a non-diseased individual as being negative.
What are the two main outcomes of positive and negative test results, and how do they relate to predictive values?
-The two main outcomes are true positives and true negatives for correct diagnoses, and false positives and false negatives for incorrect diagnoses. Predictive values help assess the reliability of these test results in determining the actual presence or absence of a disease.
How can the positive predictive value (PPV) be calculated from the provided data?
-The positive predictive value can be calculated by dividing the number of true positives (140) by the total number of positives tested (175), resulting in a PPV of 80%.
What is the issue with using a 2x2 table to calculate PPV and NPV if the data is not collected prospectively?
-If the data is not collected prospectively, such as in a case-control study design, using a 2x2 table to calculate PPV and NPV directly can lead to biased estimates, especially when the prevalence in the sample does not represent the prevalence in the population. In such cases, Bayes' theorem may be required for accurate calculations.
How can the threshold value (X) for a screening test impact its sensitivity and specificity?
-Adjusting the threshold value (X) can fine-tune the test's sensitivity and specificity. Lowering the threshold to increase sensitivity will likely result in more true positives but also more false positives, thus decreasing specificity.
What is the importance of understanding sensitivity, specificity, and predictive values in medical testing?
-Understanding these concepts is crucial for evaluating the accuracy and reliability of medical tests. They help determine how often a test correctly identifies individuals with or without a disease and are essential for making informed decisions about diagnosis, treatment, and public health strategies.
Outlines
🧪 Introduction to Screening and Diagnostic Tests
This paragraph introduces the concepts of screening and diagnostic tests, emphasizing their importance in medical diagnostics. It outlines the purpose of each test type, with screening tests used to identify at-risk individuals before symptom onset and diagnostic tests to confirm the presence or absence of a disease. The paragraph also highlights the differences in cost, invasiveness, and the intended populations for these tests. It sets the stage for a deeper discussion on the metrics of sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), and explains how to calculate these using 2x2 tables. The limitations of using 2x2 tables for calculating PPV and NPV are also mentioned.
📊 Developing and Evaluating a Screening Test
The second paragraph delves into the process of developing a hypothetical screening test, using a blood level measurement as an example. It explains how the test is designed to identify individuals likely to develop a disease before symptoms appear. The paragraph outlines the prospective nature of the test development, following a cohort of individuals over time. It provides a detailed example with numerical data, illustrating how to calculate sensitivity, specificity, PPV, and NPV. The paragraph also discusses the impact of adjusting the test's threshold on its sensitivity and specificity, and the trade-offs involved in doing so.
🚫 Limitations of 2x2 Tables in Prevalence Estimation
The final paragraph addresses the limitations of using 2x2 tables for calculating PPV and NPV, particularly when the data is not collected prospectively. It explains that if the prevalence of the disease in the sample does not represent the population, direct calculation from a 2x2 table will yield biased results. The paragraph introduces the case-control study design as an alternative method and mentions the need for Bayes' theorem to calculate PPV and NPV in such scenarios. It concludes by emphasizing the importance of understanding these concepts for accurate medical decision-making and encourages viewers to explore more instructional videos on the topic.
Mindmap
Keywords
💡Screening Tests
💡Diagnostic Tests
💡Sensitivity
💡Specificity
💡Positive Predictive Value (PPV)
💡Negative Predictive Value (NPV)
💡Prevalence
💡False Positives
💡False Negatives
💡2x2 Table
💡Threshold Value
Highlights
Screening and diagnostic tests are discussed, focusing on concepts like sensitivity, specificity, positive predictive value, and negative predictive value.
Screening tests are used to identify individuals at risk before symptoms appear, aiming for early detection.
Diagnostic tests confirm the presence or absence of a disease in symptomatic individuals or those who tested positive in a screening test.
Screening tests are typically cheaper and non-invasive, whereas diagnostic tests are more expensive and often invasive.
Screening tests have higher sensitivity and false positive rates to not miss potential cases.
Diagnostic tests should have high sensitivity and specificity to accurately confirm or refute a disease.
Positive test results from screening tests usually lead to more invasive diagnostic tests, while positive results from diagnostic tests lead to disease treatment.
The cost of screening tests should be justified, and diagnostic tests, though expensive, are necessary for confirmation.
Sensitivity is the probability of a positive test result in individuals with the disease, also known as true positives.
Specificity is the probability of a negative test result in individuals without the disease, also known as true negatives.
Positive predictive value indicates the likelihood that an individual with a positive test result actually has the disease.
Negative predictive value indicates the likelihood that an individual with a negative test result does not have the disease.
A 2x2 table is used to calculate sensitivity, specificity, positive predictive value, and negative predictive value.
The video discusses how changing the threshold value in screening tests can affect sensitivity and specificity.
The use of a 2x2 table for calculating positive and negative predictive values can be biased if data is not collected prospectively.
Bayes' theorem is mentioned as a method for calculating PPV and NPV when data is collected through a case-control study design.
The video aims to help viewers understand the importance and application of these testing concepts in a clear and practical manner.
Transcripts
Browse More Related Video


5.0 / 5 (0 votes)
Thanks for rating: